

There are two big uncertainties with COVID-19. The first is whether there will be a vaccine and if so, when it will be rolled out. The second is the proportion of asymptomatic cases for each confirmed case. This second issue will have a fundamental influence on how long will it take, both with and without a vaccine, before some level of population immunity can be reached across the globe.
Despite the huge uncertainties in relation to both a vaccine and asymptomatic infections, there is newly emerging empirical evidence in relation to each of them. I will look at each in turn.
There are also some other issues where the evidence is now more sustained and increasingly compelling. First, it is increasingly likely that genuine elimination of the disease within New Zealand can be achieved and kept that way, as long as border control remains tight. Getting it wrong at the border risks everything.
Second, there is very high likelihood that Europe and the USA will have at least one more devastating wave of COVID-19, with that wave much more devastating than the current one. It is going to be a big mess.
Third, in much of the less-developed world, including middle-income countries such as Brazil, COVID-19 is out of control and unstoppable.
More on all of those also.
There is good news with vaccines
Just this last week, American-based Moderna announced early stage success with its revolutionary messenger RNA (mRNA) vaccine trials. Many in the global media, parroting off each other, misunderstood what it was about and provided a flawed commentary, including the mistake that results were based on only eight people.
But not everyone was fooled. The big investment companies had more analytical expertise at hand than did the media, and so global share markets jumped on the day of the announcement. Within the media, there is now debate as to whether that was insight or exuberance.
First some background. Currently there are no mRNA vaccines that have been licensed for any disease. This is because it is a revolutionary technology that Moderna, and no doubt some others, have been working on for quite some time trying to sort out the wrinkles. This started long before COVID-19 came along.
mRNA is the mechanism by which the body produces protein on command from DNA. It is the process that drives all protein synthesis. Depending on the message contained within the mRNA, cells can produce any protein. This includes proteins that are specific to coronaviruses but which by themselves have no ability to cause COVID-19 or any other disease.
Moderna has now worked out how to manufacture the right type of mRNA. More importantly, they have also worked out how to transport the mRNA through cell walls and to then keep it active. The human cells then synthesise the specific protein as commanded by the mRNA.
The body then reacts to this foreign protein by producing antibodies. In this way the body is primed to attack COVID-19 virus particles containing the same protein. At that point it is close to game over for COVID-19!
So how far has Moderna actually got? The first step was to inject the specific manufactured mRNA into 45 humans and see what happened. The first piece of good news was that none of the 45 people got seriously sick, although at the very highest dose, which was 18 times the low dose, some people did get a one-day fever. The second piece of good news was that all 45 people, including all of those at the low dose, produced the specific COVID-19 protein and everyone then produced antibodies. So that means that they only need to focus on the low and medium dose rate, and can forget about the high rate.
This antibody development stage is called ‘seroconversion’. The next stage is that antibodies were collected from the first eight people in the trial and these antibodies latched onto and destroyed COVID-19 in a test tube. In scientific language, they neutralised the virus. In the next few weeks, Moderna will do this test with more seroconversion antibodies, but eight is enough to know that it definitely works, at least in the test tube.
A parallel trial has been to do the same thing with mice but taking it one step further and this time infecting those mice with COVID-19. The vaccine worked and the mice were protected from the virus.
The next step will be to repeat the process in some hundreds of humans, and then thousands of humans, each with their own individuality, testing for effective production of antibodies and looking for side effects in various sub-populations.
Purposefully infecting the humans, as was done with the mice, is a big ethical issue for any vaccine-development program. Accordingly, the alternative is to test the drug on thousands of people in countries where the disease is rampant. The reason that thousands will be needed is that this type of trial can give false results because of chance involved as to who gets exposed to the disease and who is not.
Much time could be saved if volunteers agree to be infected and if authorities allow for this to be done. Then it would only require about 20 people, purposefully infected, to see if the vaccine protects the volunteers. There would be no placebo treatment of infecting people without the vaccine, so it would not be so-called ‘gold standard’, but it would still provide a very high level of proof. With this approach, the trial could be conducted anywhere, but under strict medical supervision and quarantine, regardless of the community level of transmission.
Moderna is hopeful of having a vaccine ready for licensing by September and then rolling out production from there from late 2020 and through 2021. However, I cannot see this community roll-out starting in 2020 unless they can get ethics approval for purposeful infection.
The history of vaccine trials is very much a story of ‘what can go wrong will go wrong’. The famous Murphy of Murphy’s Law would have nodded his head sagely. So, the journey is far from over. But it is now apparent that vaccines can be manufactured that will lead to appropriate antibody production.
What the scientists now have to be sure about is that the vaccine does not also do unwanted things such as stimulating auto-immunity in some people, such that the body also attacks its own healthy cells. Also, there are big questions about how long the immunity can be maintained. These same issues will be relevant to all the competing vaccine development programs.
Another good thing with mRNA vaccines is that they will be much easier to scale up than all other types of vaccine. For example, quality assurance issues are much easier when working with mRNA than with a vaccine that relies on an attenuated virus. Yet another advantage with mRNA vaccines is that it is easier to tweak the vaccine if the virus mutates.
Even further good news is that if the COVID-19 vaccine works, then similar vaccines can be developed for many other diseases, including some genetic diseases. So, watch out for further news on mRNA vaccines relating to multiple diseases.
A cautionary note, and it is a strong cautionary note, is that all of the above is just one scenario, albeit one that is starting to look more likely. If it were a horse race, then Moderna should now be the favourite, but of course not all favourites make it down the home straight as winners. Horses from other stables will still be favoured by their owners.
The bad news is that if the Moderna vaccine fails it will be because it ‘fell over’. It won’t simply be a case of other vaccines roaring past at speed to the finish line. If obstacles appear for the Moderna vaccine in relation to either non persistence of immunity or emergence of auto-immunity, then these obstacles are likely to affect all vaccines.
There is confusion about asymptomatic cases and population immunity
One of the most contested issues associated with COVID-19 must surely be the extent of asymptomatic cases. Much of the information supplied to the public has been a total muddle.
The initial muddle was created by confusion between pre-symptomatic cases versus truly asymptomatic cases where the disease went through its whole cycle of infection and recovery without any symptoms. The situation then became even more muddled with testing criteria and protocols differing from country to country, and with testing details not explicit.
One of the key issues with antibody testing relates to what is called the ‘specificity’ of the test. This specificity determines the likelihood of false positives and it is different for each test and manufacturer.
Particularly in the early stage of a pandemic, when the number of genuine positives in a population is low, then the proportion of false positives is always likely to be high. People who did not understand these issues have extrapolated apparent but false levels of disease positivity to subsequent stages of a pandemic and this has been a false path of logic.
Here in New Zealand, we can be confident that the number of asymptomatic people capable of transmitting the disease has been low. Otherwise, we would have seen ongoing evidence for community transmission.
When looking overseas, New York City is particularly insightful. This is because the penetration of the disease there is greater than any other city that has detailed data. As of 1 May, New York City had 18,282 confirmed and probable deaths from 166,000 cases. However, a New York State Government study estimated that at that date 20 percent of the population in the city were antibody positive, which would suggest 1.7 million people had been infected. However, not all of these additional people would have been asymptomatic, with many having symptoms but not recorded by the overwhelmed health authorities. Also, some may also have been false positives.
Putting aside for a moment the issue of asymptomatic cases versus symptomatic but unrecorded cases, Worldometers has used the 20 percent antibody-positivity data, together with estimates for both recorded and unrecorded deaths, to then estimate an infection fatality rate of 1.4% at that time, but recognising that this case fatality rate would increase thereafter because of the delay in deaths.
Any further interpretations about New York City depend on further assumptions, in particular what happens to the transmission rate, R, when social interaction restrictions are removed. However, what is clear is that under any realistic version of R as being somewhere between a low of 2.5 and a high of 6 in the absence of social restrictions, then New York City is still a long way from the point where population immunity effects can start to kick in. At that stage, the disease would start to die away. Accordingly, as New York City tries to come back to normal life, there will at some stage be a new wave of illness and death, which can only be halted by a further lockdown.
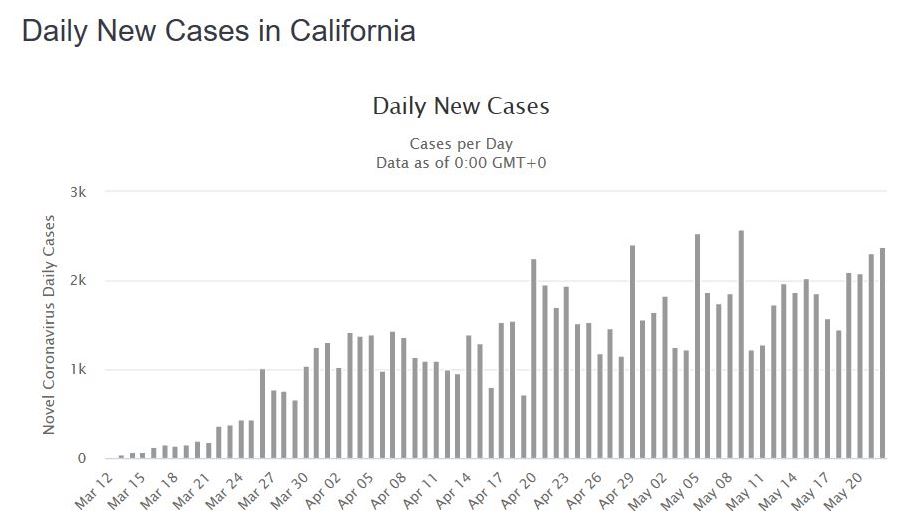
Shifting to California, where the social demography is different and the lockdown has also been less extreme, the rate of new cases has continued to rise, albeit much more slowly than occurred in New York. The story is similar for Florida. As these states now relax their lockdown policies, it seems logical that case rates are going to rise much more.
In Sweden, the policy has been very much one of flattening the curve but also trying to keep the economy going. The policy of long-term flattening the curve is so they can manage the case load until population immunity is eventually reached. A month ago, they were saying that that they thought within Stockholm, which has much higher levels of COVID-19 than elsewhere in Sweden, they would be seeing signs of population immunity by now.
In contrast, the reality of Sweden now towards the end of May is of no clear evidence of declining cases, despite restrictions broadly similar to New Zealand’s LEVEL 2. Also, on a per-capita basis, Sweden has in recent weeks had death rates higher than everywhere else in Northern Europe apart from perhaps Britain, with Britain being a great mess.
The latest advice (20 May) from Sweden’s State Epidemiologist Anders Tegnell is that he believes about 20 percent of the Stockholm population is likely to have been infected but that antibody levels are much lower elsewhere in the country.
Overall cumulative per-capita death rates in Sweden are now eighth highest across the World, some seven times higher than in neighbouring Finland and nine times more than neighbouring Norway. It is also insightful that the level of economic disruption in Sweden and the extent of recession is broadly similar to the European countries that are in lockdown. At best, it seems that Sweden must remain for a long time at the equivalent of New Zealand’s LEVEL 2.
Searching across the globe, the overarching conclusion in regard to population immunity is that so far there is no evidence of any country coming close to that position. On a global basis, it will be a long journey.
This means that, in the absence of a vaccine, combined with the reality that the world cannot remain in lockdown indefinitely, we have to date only seen the prelude, with the fugue still to come. For those unfamiliar with a musical fugue, it is where the prelude is repeated with variations and amplitude. It won’t be nice.
Even with a vaccine, it almost certainly won’t come soon enough to prevent the global fugue.
I now turn to other areas where there is increasing clarity.
New Zealand can eliminate COVID-19 with tight quarantine and a closed border
The evidence is now compelling that community transmission within New Zealand has been eliminated, at least for the meantime. The provisos relate to there being no virus leakage from the existing active cases together with maintenance of a tight border. Once again, those provisos are considerable.
It would be a tragedy if, having sailed so close to the wind back in March, but having then come though the tempest, we were now to drop our guard. Opening of the Australian border too soon, or an outbreak from airline staff not having to self-isolate, could be our undoing.
Once New Zealand opens the Australian border, New Zealand is no longer relying on its own management, but also that of Australia. Even if Australia is operating at the same level as New Zealand, by creating mobility with a population five times that of New Zealand, the risk also increases in a similar ratio.
Imagine somewhere round twenty planes per day from Australia, disgorging around 3000 people per day and close to 100,000 people per month. Twenty planes may sound a lot, but pre-COVID there were more than that number coming from Australia each day.
It only takes one of those Aussie tourists to be carrying the virus and then become infectious, and then to visit some night clubs, and the virus has spread to the four winds. At that point, New Zealand would have to go back to LEVEL 4. Why would New Zealand risk this without being absolutely sure about sustained zero rate of community transmission in Australia and not just low levels?
Europe and the USA will have ongoing waves of COVID-19 in 2020 and likely beyond
Right now, new cases are declining in most Western countries because of lockdowns. But it is only because of lockdowns. Almost all of these countries are now removing the lockdown screws despite not having stamped out the disease.
Close inspection of the data shows that in many countries the curve is already showing early signs of turning upwards again. Give things another month or two and the embers will be flaming away. What do these countries do then? In comparison, New Zealand is oh so lucky.
The debate between epidemiologists about outcomes in these countries is really only about how quickly the flames will be fanned. Singapore, Mexico and other tropical countries are showing that this virus can thrive in hot conditions and it will not be stopped by summer. My expectation is that in the Western countries the build-up might be slow and intermittent for a short period, but by October, and most likely well before, the virus fires will be raging.
COVID-19 is now unstoppable in many middle-income and most low-income countries.
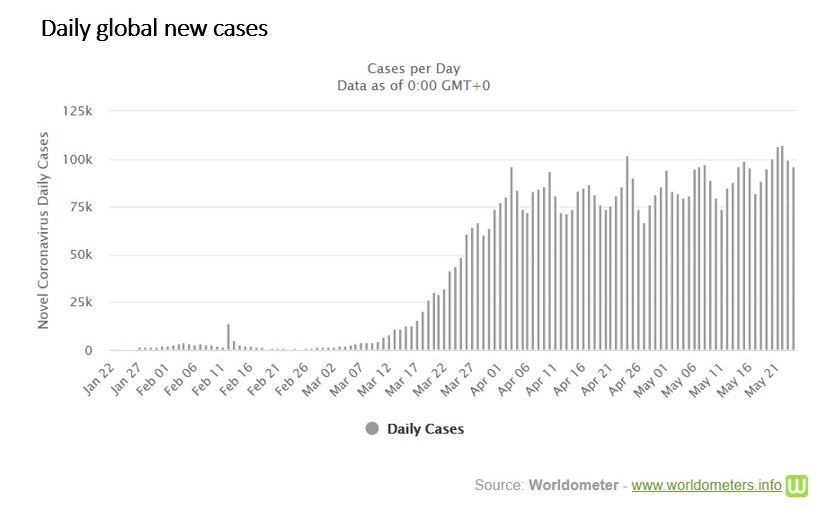
Despite Western countries reducing their COVID-19 cases under lockdown conditions, the overall trend of global new cases has been upwards for several weeks. It is currently averaging around 100,000 new cases per day. This is because the explosion of cases in middle-income and developing countries is outrunning the short-term decline in the more developed Western countries.
Brazil is the classic example of a country that ignored the risk when it had a chance. Now, it may well be that Brazil will provide the best evidence as to what happens when the curve is not flattened. Despite many Brazilian states trying to flatten the curve, the overall effect has been thwarted by President Bolsonaro having his own unique positions on COVID-19 management. It looks a big mess.
As for countries like India, Bangladesh and Pakistan, if Singapore could not control it in its migrant population – and clearly Singapore has failed in that regard – then what hope do these other countries have with their crowded conditions? They may be able to slow things down, but whether they can flatten the curve, rather than just delay the peak, is another matter.
And what about China in all of this?
In assessing the COVID-19 situation in China, it is essential to separate out health outcomes from politics. It is remarkable that China has gone so close to stamping out the disease. China continues to stamp hard on the embers, with the main focus on returnee citizens from elsewhere in the world. The key province of concern is Heilongjiang with its leaky Russian border. However, on a per-capita basis, China’s active COVID-19 levels, even in Heilongjiang are still very low. There can be no doubt that China understands the importance of continuing to stamp hard and that is exactly what they are doing.
Increasing pollution levels in recent weeks across much of China provide the evidence, with no need for any corroborating statistics from the Chinese themselves, that China is largely back to work. It is not totally back to normal, but there can be no doubt that China is in a totally different situation than Europe and the Americas, and also much of Asia.
There is a real irony that New Zealand (23 active cases), Australia (481 active cases), China (83 cases) and Taiwan (20 cases), together perhaps with Vietnam (58 cases), are the cluster of countries that may be close to eliminating the disease within their borders. Japan (2317 active cases) and South Korea (713 active cases) are the two other large countries that still have some hope, albeit distant, of COVID-19 elimination, but at this stage they are many months behind. Nearly everyone else is at best trying to flatten the curve with no hope of stamping it out without a high-powered and yet to be delivered vaccine.
It is notable that newly elected National Party leader Todd Muller has already flown a kite about re-establishing future travel relations with China. In doing so, he is building a pragmatic argument based on empirical evidence. Not everyone is going to like where that argument leads.
The big picture
It will be a long time, almost certainly at least 18 months, before New Zealand can open its borders beyond a small cluster of Australia, maybe nearby Pacific Islands, and perhaps a set of East Asian countries. New Zealand now needs to work out what its medium-term positioning might look like with much of the rest of the world in ongoing social and economic disarray.
New Zealand is in the fortunate position of having options at this time that few other countries have.
*Keith Woodford was Professor of Farm Management and Agribusiness at Lincoln University for 15 years through to 2015, and retains an honorary position as Professor of Agrifood Systems. He is now Principal Consultant at AgriFood Systems Ltd. One of his interests is the epidemiology of both animal and human diseases. He can be contacted at kbwoodford@gmail.com. Keith’s previous COVID-19 articles are available here.
86 Comments
It is very plain to me that the money we have earned in the past from exports is not going to be so freely available, so the only sensible way to compensate for that is by not importing so much.
Too bad we spent so much of the last decade or so selling the means of earning our own way in the world, from our large successful companies to our damned houses. Not having done that would have made our path to more self sufficiency far easier.
Buy NZ made wherever you can, and really think about whether you really need that imported stuff you are planning to buy.
Keep as much as we can here, I can't really see much option.
We are going to be waiting a long, long time for the rest of the world to get to where we are. We may be able to take some advantage with that (film making springs to mind).
This is out of the hands of the govt (any govt). Fortunately, because of the govt we do have, we will not have to be battling with an out of control virus, along with economic difficulties.
PocketAces,
I agree that we should be figuring out what we can do efficiently in NZ.
Bringing call centres back to NZ could be a good place to start.
Maybe NZ consumers could buy more NZ pork rather than imported?
But then it starts to get harder to find the specifc things we should be doing that don't require big subsidies.
Maybe manufacturing more pharmaceuticals?
Everyone talks about 'value-add' but it is easier to talk about than to do.
KeithW
Keith,
There seems to be a body of scientific thought that Covid will be like influenza, ie a seasonal, recurring illness. If that is correct, it will be virtually impossible to keep it out of New Zealand in the long term. I do agree that we should repatriate jobs. Perhaps an implied income tax on outsourced overseas workers would help.
Pietro
The way that COVID-19 is playing out in tropical countries suggests the seasonality issue may be different to influenza. But there may still be a seasonal issue in the same way that winter colds seem more long-lasting and severe than summer colds. Also, I do watch and read the vitamin D stories with interest. One of the reasons I never discount Vitamin D is the simple observation that evolution shows how important it is to get just the right amount of UV light (and hence vitamin D synthesis). It is not by chance that fair-skinned blue-eyed races developed in high latitudes and dark-skinned brown-eyed races developed neaar the equators, with lots of nuances in between.
I also agree that without a vaccine we would need to eventually learn to co-exist with it.
KeithW
Pietro, the great thing about having nearly eradicated SARS-Cov-2 in NZ is that we have choices that almost no other country has. We have also bought ourselves time and space to prepare, which is without question the most ideal scenario to have in a global pandemic with a novel virus. We simply don't know enough about the virus yet to claim to understand what the future will hold but global resources have all pivoted to testing, treatments, vaccines and increasing healthcare capacity and NZ will also be able to benefit from having bought time to see whether those areas might bear fruit. Improved understanding, treatment and healthcare facilities will mean the virus will be more manageable moving forward, if it does indeed become endemic. We are the envy of the world.
I guess Covid19 will mean a lot of people will lose their homes & this will provide a perfect opportunity for foreigners via proxies to buy up more Auckland housing as a safe land bank.
The ramifications of this pandemic are incomprehensible but we can be sure opportunism will eventuate
Good luck NZ
Keith, could you kindly explain where you get the 18 month+ time horizon from re opening borders outside of Oz / some Pacific islands. Im not saying it's wrong I just wondered where the number had come from.Thanks.
That will most likely just be someone's reckons, but I reckon they were dreaming
Glitzy
Like other things with COVID-19, the timeline is not set in concrete. But it does set a guideline for planning, reecognising the Eisenhower maxim along the lines of 'plans are nothing, but planning is everything'.
If the Moderna vaccine works, then it could potentially be licensed by the end of 2020.
But that is really pushing things in terms of evaluating long-term side effects and duration of immunity.
Equipment has to be built although that is starting now.
Then the vaccine has to be distributed.
New Zealand would need to get approximately 80% of its own population vaccinated before opening the borders. Even then, NZ would probably want very low case numbers in countries travellers were coming from. It is a huge logistical exercise across the globe. My understanding is that no vaccine has been developed and operationalised in less than four years, but with mRNA, if it works, then the manufacture is going to be considerably easier than other types of vaccine.
Coincidentally (as I had not seen this until after I wrote the article) Dr Anthony Fauci, who is the lead medical adviser to Trump on COVID-19 (and who regularly disagrees with Trump), did say over the weekend that now he had looked at the Moderna data in some detail he is more optimistic and quite excited, but still thinks it will take 18 months to manufacture, distribute and treat even if the vaccine does work. Fauci is always worth listening to - he has a great scientific record and he is only workng for Trump (as an eighty-year old) as a duty to his country.
If there is no vaccine then it will also be unlikely that population immunity can be reached within less than an 18 month timeframe. It may occur in some places on a shorter timeframe, particularly in countries that fail to threaten the curve, but not on a global basis.
So, on balance, I am comfortable with my statement that it is likely to take 18 months (or longer). That fits with the notion that much of the world has experienced the prelude but the fugue is still to come. However, always happy to see alternative scenarios laid out
KeithW
Unfortunately, Covid looks like have become an Endemic.
Only way to keep the virus away from NZ is not lifting up the current border restriction, and have two weeks self isolation for New Zealanders who come back from overseas travel.
China having only 83 active case is a practically a joke.
38 is a particularly auspicious number in Chinese. Perhaps it's a transposition error lol.
I hope people of influence read Keiths articles. Well researched,compulsory reading.
I suspect Keith and others just like him have made a difference to our approach to covid, we owe them a huge thank you for that.
Unfortunately the more we more we look to open up - including expand exemptions the greater the risk we are taking. This risk (and that is a risk which would make our current dire economic outlook even worse) is not just from those granted exemptions but through and increase in cabin crew etc coming in, who are not required to quarantine. I notice that recent articles on Avatar staff exemptions noted that they would be required to quarantine or self-isolate. To my knowledge everyone else is required to quarantine at the present, would be interesting if those who have been granted exemptions are also exempt from quarantine - we all know how well compulsory 'self isolation' worked in early March.
Just would like to add, not sure if I would trust figures out of China as far as I could throw them.
Believe it or not, their "Reported" confirmed cases per Capita is only a quarter of NZ's
PocketAces,
One should also at least consider the possibility that they might be broadly correct.
In all societies there is a tendency for mid-level officials to make themselves look good. Also, the fatal weaknesses of centralised authoritarian govenments is to never have enough information as to what is really happening. The damage of false data is largely to themselves as it exacerbate the problem.
China has twice dug a big hole for itself in that regard. The first time was during the time of the so-called Great Leap Forward in the late 1950s which coincided with a huge drought and led to millions of deaths. The second time was in the Cultural Revolution less than ten years later . But the Chinese learned from those experiences.
The Chinese public health system is actually very good and it is run by medical experts. Where things can go wrong is when political operatives over-ride the experts and this did happen in Wuhan in the last ten days of 2019. That slowed things down but only by about ten days at most.
The Chinese medical folk have always been in close communication with Western colleagues. The problem in the West is that we listen to the politicians (both theirs and ours) rather than listening to the people who really know.
KeithW
I concur. Seeing the trouble they have with these stats in developed countries it would be surprising if the Chinese stats are accurate or even if the Chinese medical folk would say they are accurate. What matters is they seem at present to have it under control but they still do have cases so we would have to treat visitors from China with care just as we would with similar countries that have it apparently under control: Taiwan, Australia. I do think NZ could and should open up non-quarantine travel with many Pacific countries especially those that never had a single case.
Sorry, don't trust them. Don't trust them over that or Hong Kong, or Taiwan or Tibet or the Uighurs, they are becoming far too aggressive and I think the best place to be where the Chinese govt goes, is as far away as possible. They are becoming extremely dangerous and we should not embrace becoming any more beholden to them.
Thanks Keith. I share your view that China's numbers are broadly correct. China has little to gain by obfuscating the facts, and everything to gain by maintaining its aggressive attempts to keep the virus in check. Their (health) leadership and international participation in looking for solutions stands in stark contrast to our American friends at the moment
Todd’s got to open up the borders to Beijing. Got to keep the donors happy
I thought he implied, keep borders shut .
He stated that the boarders with Oz and China need to be opened as soon as possible.
National will not be raising GST to 15%. National are about decreasing taxes, not increasing taxes.
- Sir John Key - 2008.
We will build 100,000 houses
We will plant 1 billion trees
We will reduce child poverty
We will reduce homelessness
We will...
They all lie. Every politician from every party.
Q: How can you tell an MP is lying?
A: Their lips are moving.
The 1 billion trees was over a 10 year time frame, during which time 500m trees were due to be planted. A doubling of the trees didn't seem unrealistic. Too soon to call it a lie.
There have reduced child poverty.
They have reduced homelessness.
Is that a purely government planting number as was strongly implied, or are they counting private plantings in that figure?
They have reduced homelessness by doing exactly the same thing they moaned about National doing - putting the homeless in hotels and paying massive amounts to do so. Until Covid19 hit, migration levels were still high and more people were being added than houses were.
There has been no meaningful impact in child poverty figures. Most movements in the most recent update were inside the margin of error. In some indicators, they went backwards.
Three long years of neglect.
GV,
The tree number includes private plantings. It is nothing more than a political catch cry.
KeithW
Wow, that is some irrefutable proof right there. I stand corrected and will amend immediately.
Q: How do you know a non-Labour MP is Lying?
A: Their lips are moving.
Q: How do you know a Labour MP is lying
A: Their lackies post opinion based rebuttal defending them, without any references, let alone credible ones.
Now about Kiwibuild again?
Pike river?
"Pause on Immigration" - and don't say Covid.
Tax working group (Heck any of the working group recommendations)?
Oil and Gas consultation?
no "new" taxxes, but lots of increases to existing ones.
Oh, FYI its not personal, or a Labour thing. They are all as bad, we could be here for days, weeks, month listing the lies of various parties. It's just that Labour are in power at this very moment. They also have the unfortunate start of having a PM that basically said she does not lie, so it is only fair that she should be called out to a slightly higher standard when they do lie - and they all do.
Yes she did. Bold as brass. 'I dont lie'. And the goddamn media lapped it up. Bill English, who was honest, and could not lie, said yes sometimes he has to lie. The media blasted him. I tore my hair out in frustration.
Good article
The point is that global economics is in such trouble that operating in some kind of insider's bubble will never happen. Do you think the rest of the world will stand by and collapse, while a small coterie thrive? Not going to happen. Won't be allowed to happen. The others will be at war before that.
Sadly, I do think you are right, but have been trying to think beyond that.
This virus:
"Four infectious disease doctors in Canada estimate that the individual rate of death from COVID-19 for people under 65 years of age is six per million people, or 0.0006 per cent – 1 in 166,666, which is “roughly equivalent to the risk of dying from a motor vehicle accident during the same time period.” These numbers are for Canada, which did have fewer deaths per capita than the U.S.; however, if you take New York City and its surrounding counties out of the equation, the two countries are pretty much the same. Also, remember, so much of the death is associated with the suicidal political decisions of certain states and countries to place COVID-19 patients in nursing homes. An astounding 62 percent of all COVID-19 deaths were in the six states confirmed to have done this, even though they only compose 18 percent of the national population."
https://www.zerohedge.com/health/cdc-confirms-remarkably-low-death-rate…
Rosenstein'
It would appear that these death rates are early stage deaths under lockdown.
KeithW
The shorthand label for the small set of countries we will be able to interact with is the 'Green Zone'. It will become a prized marketing tool: but all depends on the quality of border detection, the subsequent enforced and tested quarantine, and the ability to squelch any cases from leakages in any of the foregoing. That demands great vigilance and superb competence........that's a high bar for any Gubmint.....
What a great article. Highly informative, and beautifully written.
World screwed up badly not mandating universal masks, they drop infection rates to as little as 2% of no masks. Ensuring no Vit-D deficiency also saves lives. If infected make sure it's a minimal dose - a big or repeated exposure to virus is more likely to kill (eg for smallpox and measles can make 10x difference). Several countries have IFR 0.5% or less (Iceland, Singapore, Qatar), so likely only about 1 in 200 infected die, <1 in 2000 if under 40. Risk of death equal to about 4-5months of your normal life.
Masks for 8 billion people per day, often more than one per day? Where were they going to be coming from at day dot?
The supply issue is different from the 'do they work issue".
We get told 'they don't work, but we don't have enough anyway, and the ones we do have have to be kept for healthcare workers.' What a contradiction.
Apparently sneezing/coughing into your elbow works, but masks don't.
Yes agree, but according to this Govt., they don't work, otherwise, they would be using them.
If they were looking at most successful countries, one of the denominators is they wear masks.
Alert level 2 alert plus the wearing of masks (which would have also allowed for social distancing to be reduced or stopped) and international controls, contact tracing would have been all that was needed rather than Alert level 4.
Even now, masks on public transport would allow twice the density.
Foyle,
I agree with your point that the inital virus dose is important. I believe this is why so many health workers have died. They get a big initial dose of the virus and their immune systems do not have enough time to crank into action. I would very much like to see a separate study of health workers. These are the people across the globe who are carrying the burden and putting themelves in situations of self-risk. Some weeks back - probably now about four weeks ago, perhaps longer - there had already been approximately 90 health care professionals and a similar number of health carers who had died of COVID-19 in the UK alone.
KeithW
One study showed that the highest concentration of virus particles was in the changing area where the health care workers get in and out of their PPE.
HVAC ventilation flow patterns within the building also had a big impact on virus concentrations.
The flow pattern becomes important, subject to how airborne the virus can become. And how airborne it becomes is set by temperature and relative humidity https://40to60rh.com/
In a post restaurant study in Wuhan were certain diners got infected, and others didn't, plus no staff were infected (just like the Bluff wedding reception) is was shown that ventilation flow correlated to where those that got infected and were within that zone for at least fifteen minutes.
Do lockdowns work?
https://wmbriggs.com/post/30833/
to quote:
'Nature gets no credit. Not for the creation of the virus, not for its highly variable spread, not for its highly variable infection rate, and certainly not for its hugely variable deaths caused. All those things were believed to be the responsibility of people. Nature has no real power, we think. It can be controlled to any degree of precision desired, if only we can muster sufficient political will and suppress our enemies.
We can credit, as we’ve already seen, the lockdowns for causing any number of difficulties, such as massive job loss, grief, disharmony, terror, and even death. It cause hubris to rise to the bursting point.'
NZ, and (Australia not having a lockdown anywhere like NZ so as to be not a lockdown), has so far dodged a bullet more because we are low-density comparatively speaking and are out of season for most viral infections.
We have no herd immunity or controlled community transmission and are the equivalent of the native populations before the first Europeans turned up with their diseases that no one had immunity for.
We have just about to enter our virus season, so if the virus is about, then we would expect a natural increase, just like the flu. And if that happens and we can keep it within our hospital's capacity to handle it, then it is not an all or nothing response back into level 4.
Florida has not had one documented case attributed to any outdoor infection. Almost all infections worldwide have happened within buildings.
Personally I dont think the future is clear at all its way to early to even start predicting an outcome or scenario. Its only getting started in several countries and I have little faith in a vaccine and sure will not be lining up to get it.
"I have little faith in a vaccine and sure will not be lining up to get it."
Just out of interest; why not?
One possible reason...this is what happened last time a vaccine was rushed through:
Brain-Damaged UK Victims of Swine Flu Vaccine to Get £60 Million Compensation
https://www.ibtimes.co.uk/brain-damaged-uk-victims-swine-flu-vaccine-ge…
Really good article again Keith.
My concern with having a travel bubble with Australia, is that Australia seem to also want to have a travel bubble with other countries , as per https://7news.com.au/travel/coronavirus-travel-bubble-could-be-expanded… . A travel bubble with just NZ and a few pacific islands, isn't really going to benefit Australia very much, compared to the benefits NZ and the pacific islands get.
I wonder if countries should get a COVID19 elimination certification from the WHO, to prove a country has eliminated it first, and has processes in place to stamp any new cases out, before opening up borders to that country, is a good idea? I also think we should be looking into special quarantine hotels/retreats now for tourists who are prepared to spend a month or more here. But I think we still need to be slective wth those countries we let in, do there is still nearly a zero chance of anyone with eh virus getting in. The last thing quarantine hotels would want are a lot of people getting sick.
Really, not sure a certificate from the incompetent WHO would be worth anything.
They have not managed any aspect of this crisis correctly and if anything look compromised and incompetent.
So glad to have you and donald to rely on for your intuitive expertise in this subject.
Nothing to do with Donald, just look at the fact of timing, its quite clear if you open your eyes.
Look at Taiwan's warning and timing of WHO announcements, they were frowning on travel bans.
It is quite clear to everyone who has been following things that WHO were primarily serving the PRC's interests, not world health, during Jan and Feb 2020.
Some of the mistakes made by the WHO:
Ignored Taiwan’s COVID warning in December
Said there was no human-to-human transmission
Said that asymptomatic transmission was very rare
Delayed declaring a pandemic
Said not to close borders
Said there was no point in wearing masks
Two Sydney schools closed yesterday after positive tests - https://www.abc.net.au/news/2020-05-26/nsw-coronavirus-case-at-sydney-school-waverley-college/12284242
Gareth
Each time I see data like that I hope that our Prime Minister also sees it.
It would be such a tragedy if we got it wrong at this stage havng come so far.
KeithW
NZ’s borders have always been open to high value customers and still are. Hundreds of foreigners have already been allowed through our “supposedly” closed borders, such as key production crew for the Avatar sequels. Many other foreigners have also been allowed through. International students, many from China, are expected to arrive in the not too distant future in a special exemption scheme currently under review.
The government has been fairly quiet on these matters, as transparency under such circumstances could possibly damage their re-election chances. One of the reasons that the general public are being held longer in lockdown, is because of the risk of a second wave starting, but not from clusters within NZ, more so from the exempt foreigners coming into the country. With only a couple of government officials calling the shots, it’s fairly easy for a very popular Jacinda to sell lockdown to the public and get away with it, at the moment.
Don't forget the airline crew with quarantine dispensation.
I guess we are all happy to live in fear and with restriction even though there is no community transmission.
There is a need for an article about how NZ handles those who cross our border. Not unexpectedly we have film makers with the ear of the govt alllowing production crew for Avatar in while we daily read of heart-rending cases of separation enforced by the same govt.
Obviously NZ has to allow its own citizens and residents to return and eventually students will return (hopefully for serious education this time not low paid work) and air cew and critical technical staff. Our economy depends on trade and that depends on some level of foreigners coming and going.
There is a big difference in risk between say a group of English rugby fans following their team from city to city and say an elderly person visiting a dying family member in rural NZ.
My suggestion is permitting foreigners into NZ without quarantine if they are from low risk countries (say Taiwan, Japan, Korea) are visiting for a low Covid-19 risk activity - visiting family, mountain climbing, carry a tracker for 14 days and make themselves conspicous - for example a headband, scarf, wristband or facemask in a distinctive colour (yellow and white stripes). It could include the numer of days they have been in NZ. Then as a nervous high risk New Zealander I could avoid them if I wished.
Great summary Keith, but I think you missed a couple of things.
First, the concern that herd immunity is a long way off misses the point. International studies are consistently showing between 1-5% of people outside cities have been infected, and 10-20% (sometimes more) within cities. Sure, these figures are less than needed for herd immunity - but they also mean that the disease is far less deadly than first thought, which makes herd immunity less critical.
Second, there's a massive age difference in death risk that is never reported. For example, if someone in their 40s catches the virus they have at LEAST a 99.9% chance of survival, and the risk continues to drop with age (and is almost non-existent for children under 15).
On the other hand, the disease can certainly be deadly for people aged 65+ with certain pre-existing health issues - hence the large number of global deaths. The median age of death is around 80, and a large proportion of deaths have occurred in rest homes - unfortunately neglected by governments in their rush to lock down entire populations.
You raise concerns about the accuracy of antibody tests (without noting that PCR tests also have issues), but the latest tests from Roche are extremely accurate, and most studies have controlled well for the limitations in the earlier tests. Further, the consistency of results across multiple countries by multiple different universities suggests the conclusions are correct.
Some sources.
The age differences in death risk were modelled long ago, at the start of lockdowns (see Table 1):
https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(20)3024…
The CDC lists the case fatality rates for different ages in the US (multiply by 0.65 for the infection fatality rate):
0-49 year-olds: 0.05%
50-64 year-olds: 0.2%
65+ years-old: 1.3%
https://www.cdc.gov/coronavirus/2019-ncov/hcp/planning-scenarios.html
There are now numerous antibody studies, some of which are listed here by epidemiologist Simon Thornley:
http://www.covidplanb.co.nz/our-posts/what-you-need-to-know-about-covid…
Using your data apply can you estimate my risk: aged 71, high blood pressure, arrhythmic heart, 3 stents and then my wife aged 59 recovering from breast cancer with full treatment masectomy, chemotherapy and radiation therapy or my 33 year old daughter being treated for an auto-immune disease?
If someone survives which is the very high probability then they are not fatal but have they recovered? Is their any data for survivors being left with new or worsened medical conditions?
Lapun,
There is no data. But there are concerns. It is yet another of those uncertainties.
KeithW
There is enough data to make a guess and there certainly are concerns. I'd put my chances of surviving getting Covid-19 about 50% and with a wild degree of uncertainty, say 5% to 95%. However we will never know unless a large sample of 71 year old volunteers with heart issues are willing to be guinea pigs.
I'm 71, retired and had a good life so not in the least panicked about myself. However my wife is young and deserves another 30 years of life; she also is working and paying taxes - do not let an average 0.26% fatality rate allow our govt to take chances with her life.
HistoryRepeats
One of the problems with antibody tests is that you cannot correct for an unknown level of specificity. To measure the specificity one really needs stored blood samples from pre-COVID days. These are widely availabe but have not been widely used. The two cities with high seropositivity that we know about are New York City and Stockholm, and almost certainly that data has broad validity in relation to the situation in those cities. Other studies, such as the Santa Clara one, are of no value ( in fact they have done damage by leading people astray) because of both inadequate knowledge as to test specificity and also a greatly flawed testing protocol which drew in people who thought they might have had the disease. If the Roche test does truly have 99% specificity then it can be of great use when used overseas to understand the population epidemiology, but still probably of lesser value in NZ at this time. Nevertheless, I have been an advocate since very early on for NZ to get organised with serology (antibody) tests to use in screening. I have also mentioned many times in previous articles how PCR tests have their own major limitations with false negatives and hence the value of using PCR and antibody tests alongside each other in specific situations.
In the absence of a vaccine, then flattening the curve and eventual (but less than total) population immunity is the only strategy. But I remain hopeful about a vaccine. And in the meanime I am oh so pleased to be in NZ.
KeithW
This article is a good contrast to much of the reportage on the possibility of a Trans Tasman travel bubble. Clearly much of the push for a travel 'bubble' has come from Travel industry lobbying. I suspect that the extent of focus on 'travel bubbles' is actually harmful in the longer term as we would be far better placed transitioning many businesses and workers out of tourism and using economic resources to facilitate this - rather than giving hope to tourism business owners and workers, which unfortunately may turn out to be a false hope.
IMO one of the biggest factors for NZ's low covid numbers is the weather. We have had a long hot summer with very high sunshine hours that was followed by a very long Indian summer autumn, also very warm with very high sunshine hours. Sunlight kills virus!
It is not just your IMO, it's fact.
Viruses are seasonal because viruses are most infective at a certain temp. humidity, sunlight levels etc.
NZ is out of season for the rapid spread of viruses. That only just starts as the cold kicks in, and you are correct, we have had very mild autumn.
And the reason is that when the weather is cold, we warm up our houses, the relative humidity can drop below 40% which is into the zone that viruses are most infective and that our human immune system is not as effective. This on top of our very poor ventilation rates makes the interior of our buildings great places to help 'catch' something. https://40to60rh.com/
And as you point out, indoors we also get less sunlight, less UV, and infrared radiation which kills viruses as well.
Other things like general health and co-morbidity issues are just a multiplier on the baseline set by our surrounding indoor environment.
Yet when have you heard anyone in NZ talking about the quality of the indoor air space in NZ buildings.
All most all infections of CV19 have happened indoors. Florida cannot find one infection that happened outdoors.
But Singapore and Mexico?
Good point.
Mexico is colder and drier and less humid than you give it credit for eg its only 11% RH in Mexico city at the moment. https://weather.com/weather/today/l/19.43,-99.13?par=google&temp=c. That's almost as low as airplane cabins get to.
Singapore's issue is that it was the poor seasonal workers that they allowed back into overcrowded conditions that were the problem. There is a big difference between crowding and density in outcomes.
But there are a couple of other factors that people are overlooking. You can catch it in one area where the conditions are ideal for catching it and then transport it to another area where you start showing the symptoms and are tested, and then that location gets flagged as the infection spot when it was not.
Secondly, people do not have receptors to 'feel' humidity levels, so the irony of what happens in many humid places where they have airconditioned offices is, in cooling down the office they also dehumidify the air so there is no condensation on the windows and in the structure, but it is dehumidified too much for the benefit of humans, ie it is taken below 40% RH. Anything below 40% is where viruses are more infective both in their survivability and there ability to be spread further as they can become more airborne.
It is common in humid countries for workers in air-conditioned offices to catch colds etc. in the middle of summer when it is hottest outside and they crank up the air conditioning. In these types of environments people avoid the summer outdoors like we avoid the winter outdoors.
It is how we set our indoor environment in response to our outdoor environment, which makes us most susceptible to catching a virus.
And we are not even talking about it. It's the same nonthought process that allows us to continually build substandard houses.
Another great article Keith. You have been consistently accurate with your assessments (and predictions) of the nature of Covid19. I think this article should be compulsory reading for anyone who wants to understand the state of play right now.
How about setting up manufacturing / Service/ Operational hub moving in direction of self reliant (where possible) and to establish this hub away from main city centre for other region to develop.
NZ can be silicon valley of the future. Problem is no one in NZ is able to think beyond China as they equate Growth = China and should not forget China will and should have China first policy and being dependent on them will get leftover (For many even that will be prosperity but at what cost to the nation)
Not to dismiss the science, but don't get lost IN the science, or distracted by it either. There's far more going on that needs attending too. Applying the 'cause and effect' analysis to the entire Covid affair leaves me highly concerned at what the outbreak has actually enabled Governments and business to do, many things that would not have been entertained EVER in relatively normal circumstances have been legitemised. Some of which I fear, may have some rather nasty longterm impacts.
Absolutely, there are extremely broad social implications from what has just happened in NZ. It's going to take years to unpick this stuff. Sudden redundancies. Unilateral wage reductions in an already low-wage economy. A huge divergence in job security and remuneration between the public and private sectors. The viewing of all work through a white-collar 'just work from home' lens, when for many it just meant 'no paid work'. The 'newly unemployed' benefit payment which is temporary, which strongly implies people not on it are not 'temporarily' out of work.
I'm not sure where to even start with any of this. It's almost all bad.
Well here is a first! I actually totally agree with you! We should be back at level 1 now! That would halt most of the shonky business practices. However the population needs to reject NOW the control freak central government rulings and get on with our lives!
Actually whilst the economic outlook is not good, unfortunately ongoing government intervention in our lives, economy, how people interact and who can come here will be required for a very long time yet. Without that ongoing intervention we would be in a much worse place. Level 2 is so diluted from what was originally proposed that I am not sure what the issue is in staying at this level...doesn't really seem much different to Level 1 anyway.
News has it that Wuhan had 200 asymptomatic cases after testing over a million people. The question is, were those 200 still active, or have their spreading vectors already moved on?
As discussed above dosage is important. A serious case of Flu gives off 11 billion virus particles per day. What if these asymptomatic cases give off just one particle? Still active but not dangerous. And on the spectrum between 1 and 11 billion where would we declare dangerous?
Where are the mitigations on key risk areas?
i.e. Face masks for elderly and tight controls on rest homes + staff + extended staff families?
Should we not be putting ongoing basic mitigations in place for these people? without shutting the country down? surely this would prevent contagion for the most vulnerable
Clearly borders and rest homes were our archilles heel and where most of our 21 deaths occurred, this was well known at the start of the outbreak
The chance of you contracting this virus and dying if you are healthy and under 60 is miniscule - the likelihood is probably on par with dying from a car accident, or the normal flu, or a bee sting or even a shark attack
i.e. tiny.... 1 in 1,000 at best and this is for most of the working class - who have lost jobs, or have reduced incomes and who also pay most of the taxes that support the countries infrastructure
This govt that has caused so much financial damage to the economy that has inevitably flowed into social issues as well - the true cost of Labours decisions is still unknown, Yet we can be certain it is massive
I kind of agree with the opportunities party that we need a constitution that outlines and protects citizens key rights that cannot be altered easily - as lock down has trodden on every bodies civil rights with people reporting neighbours or getting punished for meeting friends or going surfing which was all relatively unchallenged.... which IMO is a concern - that civil liberties can be taken away so easily
Stellar article again.
Should be sent to Winston Peters, Goff and Hipkins, who are fixated on border openings
We can't afford another level 4 due to reinfection; just have to accept that tourism and students are off the menu for a long time.
Great article. One of the few I have bookmarked.
I still think that we would be very foolish to equate Australia's level of control to ours. They have an average of about 15 cases per day and about 500 active cases. - no where near our standard. They have plateaued and remain a significant risk to us and in no way should the borders be open to them until 28 days after their last active case has recovered. (I doubt that that will happen until they have a vaccine.)
Keith, why is Belgium not spoken about when referring to COVID - it has by far the highest death rate per 1m population and also highest cases per pop according to Worldometer. Why do you say Britian is a mess? Was talking to family in the UK last night and their local hospital Royal Surrey, hasn't had any new admissions for days now as hasn't another Surrey hospital. The R factor in this area is 0.7. Rather than say Britain is a mess could it not be more correct to say parts of Britain are a mess. Family friend who is a hospital Dr in London area said that at no time were they stretched due to COVID admissions - they never got the number they were expecting. They are now returning to normal rosters due to lack of admissions.
https://www.getsurrey.co.uk/news/surrey-news/nhs-patient-coronavirus-de…
Because it's about the politics of personally as some people don't like Boris. The same way they talk about the USA as though it was one big Covid mess rather than looking at NY and other places.
Thank you Keith. And to the posters. It all makes for interesting reading, which is 10 times better than the msm paper, radio & tv does. [I'm being conservative.]
While vaccine work runs at pace, we and many others rely on contact tracing, testing and isolation case management.
Is there any news on the condition of NZ contact tracing system, this is separate to the App. News since 23rd April is hard to find.
https://www.tvnz.co.nz/one-news/new-zealand/cracks-starting-show-in-nzs…
However this example of MoH IT complements the poor performance reviews of the App.
https://i.stuff.co.nz/business/121610487/why-the-nz-covid-tracer-app-ma…
https://www.rnz.co.nz/news/covid-19/417158/government-s-contact-tracing…
https://www.rnz.co.nz/news/covid-19/417147/contact-tracing-a-very-signi…
Yes, there is clearly a risk that re-opening our border, even if only to Australia, would result in a spike in cases and inevitability, deaths. BUT, risks surely also lie in the other direction. This, I think, has been given insufficient weight. What has largely been missing from the debate are the health implications of sustained long-term mass unemployment.
I have looked at a number of studies which show very clearly the increase in mental and physical health problems that arise from unemployment. Sadly, suicides rates will rise. I don't know just where the balance of risk lies, but what must be acknowledged is that as we move forward, there is NO risk-free option.
As a long retired 75 year old, my concern is not personal, but for my sons, their families, their generation and beyond. I cannot imagine what the future must look like for many young graduates with high student debt and a rapidly shrinking job market.
Opening the border with Australia is not going to create lots of work. We are in this with the rest of the world, and any fillip the economy gets from any opening up will be shortlived as the rest of the world sinks into depression as well. Best thing we can do, is everything we can to uncouple ourselves from foreign corporations that run this country from parking cars (Wilsons) to picking up the rubbish (Waste Management) to even our iconic brands now owned by foreign corporations.
We have to look after ourselves.
You should be more worried about the prospect of world war again, and/or us being swallowed by Communist China.
We welcome your comments below. If you are not already registered, please register to comment
Remember we welcome robust, respectful and insightful debate. We don't welcome abusive or defamatory comments and will de-register those repeatedly making such comments. Our current comment policy is here.